Understanding Postpartum Depression: Causes, Symptoms, and Support

Understanding Postpartum Depression: Causes, Symptoms, and Support
December 2
Becoming a mother should be one of life’s most joyful experiences, but for many women, the postpartum period brings unexpected darkness. Explore the causes and symptoms of postpartum depression, and discover essential support strategies for new mothers.
Key Takeaways
Postpartum depression affects 1 in 8 new mothers and is more severe than baby blues, lasting weeks to months rather than days
Transcranial Magnetic Stimulation (TMS) offers a breakthrough, non-invasive treatment option that’s safe for breastfeeding mothers
TMS therapy shows 70-80% success rates in treating postpartum depression without systemic side effects
Early intervention within the first year after childbirth significantly improves outcomes for both mother and baby
Unlike traditional antidepressant medications, TMS doesn’t affect breast milk and can be combined with therapy for optimal results
What is Postpartum Depression?
Becoming a mother should be one of life’s most joyful experiences, but for many women, the postpartum period brings unexpected darkness. Postpartum depression is a serious mental health condition that affects approximately 10-15% of new mothers within the first year after giving birth, though actual rates may be significantly higher due to underreporting and stigma surrounding maternal mental health.
Unlike the temporary emotional fluctuations many new mothers experience, postpartum depression is a debilitating mood disorder that significantly impairs daily functioning and the ability to care for oneself and one’s baby. This condition can affect birth mothers, adoptive parents, and even surrogates, demonstrating that hormonal changes during pregnancy and childbirth are just one piece of a complex puzzle.
The impact of untreated postpartum depression extends far beyond the mother’s wellbeing. Research consistently shows that when mothers experience postpartum depression, it can affect infant development, mother-infant bonding, and family dynamics. Early recognition and appropriate treatment are crucial for protecting both maternal and child health outcomes.
It’s important to understand that developing postpartum depression doesn’t reflect personal weakness or inadequate parenting skills. This is a legitimate medical condition with identifiable risk factors and effective treatments available.

Symptoms and Types of Postpartum Mood Disorders
Understanding the spectrum of postpartum mood disorders is essential for early recognition and intervention. The severity of symptoms can range from mild, temporary emotional changes to serious mental health conditions requiring immediate treatment from a mental health professional.
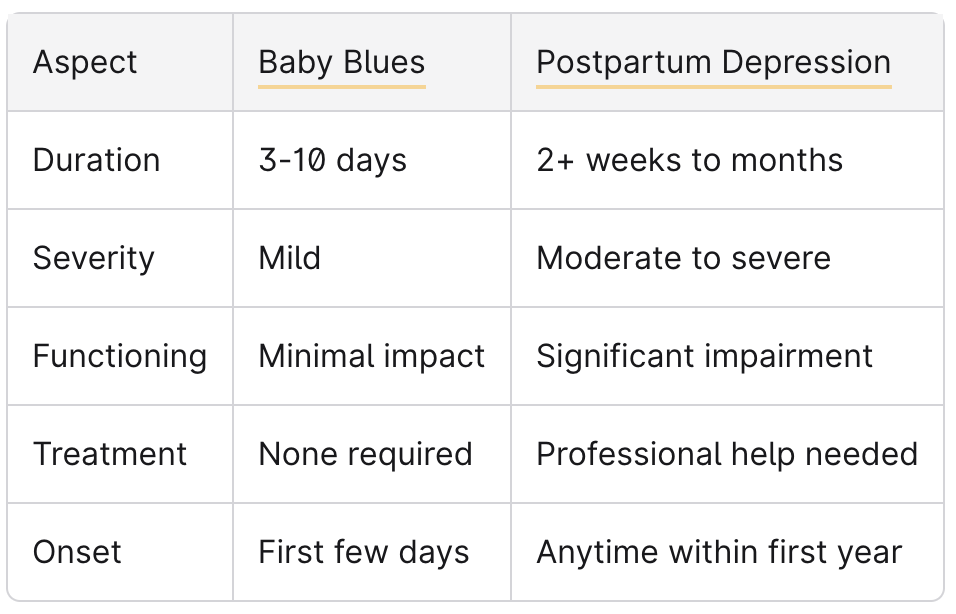
Baby Blues vs. Postpartum Depression
Many new mothers experience what’s commonly called the “baby blues” or “postpartum blues” - a mild, temporary condition affecting up to 75% of women who have recently given birth. Baby blues symptoms typically include mild mood swings, crying spells, anxiety, and difficulty sleeping. These symptoms usually emerge within the first few days after delivery and resolve naturally within 3-10 days without requiring professional intervention.
In contrast, symptoms of postpartum depression are more severe, persistent, and disabling. While baby blues symptoms are manageable and don’t significantly interfere with daily functioning, postpartum depression symptoms persist for at least two weeks and often require treatment from a mental health provider.
When symptoms persist beyond two weeks or significantly impact your ability to care for yourself or your baby, it’s time to seek evaluation from a healthcare provider.
Postpartum Depression Symptoms
The symptoms of postpartum depression encompass emotional, physical, behavioral, and cognitive changes that distinguish this condition from normal postpartum adjustment challenges.
Emotional symptoms often include overwhelming sadness, severe anxiety, guilt about not being a “good enough” mother, and feeling emotionally disconnected from the baby. Many women describe feeling like they’re drowning or trapped, experiencing intense mood swings that feel impossible to control.
Physical symptoms frequently involve persistent fatigue that doesn’t improve with rest, significant changes in appetite and eating patterns, trouble sleeping even when the baby is sleeping, frequent headaches, and various unexplained aches and pains throughout the body.
Behavioral symptoms can include difficulty bonding with the baby, withdrawal from family and friends, trouble making decisions, and being unable to complete everyday tasks that were previously manageable. Some mothers may become overly anxious about their baby’s health, while others might feel detached and struggle with emotional attachment.
Cognitive symptoms often present as severe difficulty concentrating, memory problems, racing thoughts, and intrusive worries about the baby’s safety or one’s ability to be a good parent. Some women experience baby recurrent thoughts about death or dying, which can be particularly distressing.
Postpartum Psychosis
Postpartum psychosis represents the most severe form of postpartum mental disorders, affecting approximately 1 in 1,000 women who give birth. This condition typically develops within the first few days to weeks after delivery and constitutes a psychiatric emergency requiring immediate treatment.
Symptoms of postpartum psychosis include hallucinations (seeing or hearing things that aren’t there), delusions (false beliefs), severe mood swings, confusion, and disorganized thinking. Women experiencing postpartum psychosis may have thoughts of harming themselves or their baby and require immediate hospitalization for safety.
There’s a strong correlation between postpartum psychosis and personal or family history of bipolar disorder or other mood disorders. Women with these risk factors should discuss prevention strategies with their healthcare providers during pregnancy.

Causes and Risk Factors
The development of postpartum depression involves a complex interplay of biological, psychological, and social factors. Understanding these contributors helps explain why some women develop this condition while others don’t, and why certain individuals face higher risk.
Hormonal factors play a significant role in postpartum depression development. The dramatic drops in estrogen and progesterone levels following delivery create a neurochemical environment that can trigger depression in vulnerable individuals. These pre pregnancy levels take months to normalize, creating an extended period of hormonal instability.
Additionally, thyroid dysfunction affects 5-10% of postpartum women. Postpartum thyroiditis can cause symptoms similar to depression, including fatigue, mood changes, and difficulty concentrating, making accurate diagnosis challenging.
Genetic predisposition significantly influences postpartum depression risk. Women with a family history of depression, bipolar disorder, or other mental disorders face substantially increased risk of developing postpartum depression. Having a personal history of depression, particularly previous episodes during pregnancy or postpartum periods, doubles the likelihood of experiencing postpartum depression in subsequent pregnancies.
Environmental and psychosocial factors include inadequate social support, relationship problems, financial stress, and stressful life events during pregnancy or after delivery. Women experiencing domestic violence, those without strong support networks, or those facing significant life changes alongside new parenthood face elevated risk.
Medical risk factors encompass complications during pregnancy or delivery, preterm birth, infants requiring intensive care, gestational diabetes, and certain birthing experiences. Sleep deprivation, an almost universal experience for new parents, both contributes to and exacerbates postpartum depression symptoms.
Traditional Treatment Options
Conventional approaches to treating postpartum depression typically involve a combination of psychotherapy, medication, and support interventions. While these treatments can be effective, they also present unique challenges for new mothers, particularly those who are breastfeeding.
Psychotherapy represents the first-line treatment for many cases of postpartum depression. Cognitive behavioral therapy helps women identify and change negative thought patterns contributing to depression symptoms. Interpersonal therapy focuses on improving relationships and communication skills, which can be particularly beneficial during the major life transition of new motherhood. Both approaches have strong research support for treating postpartum depression.
Antidepressant medications, such as selective serotonin reuptake inhibitors (SSRIs), are commonly prescribed for moderate to severe depression. However, antidepressant treatment in breastfeeding mothers requires careful consideration of potential effects on the infant. While many antidepressants are considered relatively safe during breastfeeding, some mothers prefer to avoid medication altogether due to concerns about infant exposure.
Support groups and peer counseling provide valuable connection with other mothers experiencing similar challenges. Support group participation can reduce isolation and provide practical coping strategies from women who have successfully navigated postpartum depression.
Lifestyle interventions include establishing consistent sleep schedules (as much as possible with a newborn), regular physical activity, proper nutrition, and stress management techniques. While these approaches alone may not be sufficient for treating clinical depression, they serve as important adjuncts to professional treatment.
The primary challenges with traditional treatments include medication side effects, concerns about infant exposure through breast milk, treatment resistance in some individuals, and the time required for antidepressants to become effective (typically 6-8 weeks).

Transcranial Magnetic Stimulation (TMS) for Postpartum Depression
Transcranial Magnetic Stimulation represents a revolutionary advancement in treating postpartum depression, offering hope for mothers seeking effective treatment without the concerns associated with medication. This FDA-approved, non-invasive brain stimulation therapy has emerged as a game-changing option for women struggling with moderate to severe postpartum depression.
How TMS Works for Postpartum Depression
TMS therapy uses precisely targeted magnetic pulses to stimulate specific brain regions associated with mood regulation. The treatment specifically targets the left dorsolateral prefrontal cortex, an area that often shows decreased activity in individuals with major depression.
During postpartum depression, hormonal fluctuations and stress can disrupt normal neural activity patterns in mood-regulating brain circuits. TMS works by delivering focused magnetic fields that penetrate approximately 2-3 centimeters into the brain tissue, generating small electrical currents that help restore normal neural firing patterns.
Unlike systemic treatments, TMS directly targets the source of depression in the brain without introducing medications into the bloodstream or affecting other body systems. This targeted approach makes it particularly appealing for new mothers concerned about exposing their infants to antidepressant medications through breast milk.
Benefits of TMS for New Mothers
The advantages of TMS therapy for treating postpartum depression are particularly compelling for new mothers navigating the challenges of caring for an infant while managing their mental health.
Breastfeeding safety represents perhaps the most significant benefit for many new mothers. Since TMS doesn’t involve any medications entering the bloodstream, there’s no risk of drug transfer through breast milk. This allows mothers to continue breastfeeding without concerns about infant exposure to antidepressants.
High success rates make TMS an attractive treatment option. Clinical studies show that 70-80% of patients with postpartum depression experience significant improvement with TMS therapy, with many achieving complete remission of symptoms. These success rates are comparable to or better than traditional antidepressant treatment.
Minimal side effects distinguish TMS from medication-based treatments. The most common side effects are mild headache or scalp discomfort during or immediately after treatment sessions. These effects typically decrease as patients become accustomed to the therapy and rarely lead to treatment discontinuation.
Rapid onset of improvement provides crucial relief for struggling mothers. While antidepressant medications typically require 6-8 weeks to show full effects, many TMS patients begin experiencing mood improvements within 2-3 weeks of starting treatment.
Preserved cognitive function is particularly important for new mothers who need to remain alert and focused for infant care. Unlike some antidepressant medications that can cause “brain fog” or concentration difficulties, TMS doesn’t impair cognitive function.
Compatibility with therapy allows for comprehensive treatment approaches. TMS can be effectively combined with psychotherapy, support groups, and other non-pharmacological interventions to optimize treatment outcomes.
TMS Treatment Process
Understanding what to expect from TMS therapy helps new mothers make informed decisions about this treatment option and prepare for the commitment involved.
The process begins with an initial consultation where a mental health professional evaluates the patient’s symptoms, medical history, and treatment goals. During this appointment, the provider determines whether TMS is appropriate and explains the treatment protocol.
Brain mapping occurs during the first treatment session to identify the optimal location for magnetic stimulation. Using specialized equipment, the technician locates the motor cortex by delivering magnetic pulses and observing hand movements, then uses anatomical measurements to target the appropriate area for depression treatment.
A typical TMS course involves 30-36 treatment sessions delivered over 6-8 weeks, with five sessions per week during the acute treatment phase. Each session lasts approximately 20-40 minutes, during which patients sit comfortably in a specialized chair while the magnetic coil delivers precisely timed pulses.
Patients remain fully conscious and alert throughout treatment and can resume normal activities immediately afterward. Many mothers arrange childcare during sessions or, in some cases, bring their infants to appointments if the treatment facility accommodates this arrangement.
Maintenance treatments may be recommended to prevent relapse. These typically involve periodic sessions (weekly or monthly) for several months following the initial treatment course, though the specific schedule depends on individual response and risk factors.
Insurance coverage for TMS has expanded significantly in recent years. Many insurance plans now cover TMS for treatment-resistant depression, though coverage criteria and prior authorization requirements vary. Treatment facilities often assist patients with insurance verification and appeals processes.

When to Seek Help
Recognizing when postpartum emotions have crossed the line from normal adjustment challenges to clinical depression requiring professional intervention can be difficult, especially for first-time mothers who may not know what to expect during the postpartum period.
Warning signs requiring immediate medical attention include any thoughts of harming yourself or your baby, inability to care for your basic needs or your infant’s needs, hallucinations or delusions, and severe anxiety or panic attacks that interfere with daily functioning. If you experience any of these symptoms, contact emergency services immediately or call the suicide and crisis lifeline at 988.
Symptoms persisting beyond two weeks after delivery warrant evaluation by a healthcare provider, even if they seem manageable. Early intervention significantly improves treatment outcomes and prevents symptoms from worsening over time.
Healthcare providers to contact include your obstetrician-gynecologist, primary care physician, or a mental health specialist with experience in perinatal mental health. Many women start by discussing concerns with their OB/GYN during routine postpartum visits, as these providers are familiar with postpartum mental health issues.
The U.S. Preventive Services Task Force recommends routine depression screening for all adults, including postpartum women. Tools like the Edinburgh Postnatal Depression Scale are specifically designed to identify postpartum depression and can help healthcare providers assess symptom severity.
Emergency resources include the National Suicide Prevention Lifeline (988), Postpartum Support International’s helpline (1-800-944-4773), and Crisis Text Line (text HOME to 741741). These resources provide immediate support and can help connect you with local mental health services.
Remember that seeking help demonstrates strength and commitment to your family’s wellbeing, not weakness or failure as a mother.
Prevention and Support Strategies
While not all cases of postpartum depression can be prevented, research has identified several strategies that can reduce risk and improve outcomes for new mothers and their families.
The U.S. Preventive Services Task Force recommends that healthcare providers refer pregnant and postpartum women at increased risk for perinatal depression to counseling interventions. High-risk factors include personal or family history of depression, current depression or anxiety symptoms, stressful life events, and limited social support.
Prenatal mental health planning involves discussing mental health history with healthcare providers during pregnancy and developing a plan for monitoring and support during the postpartum period. Women with previous episodes of depression should work with their providers to establish early intervention strategies.
Building support networks before delivery provides crucial resources during the challenging early weeks of parenthood. This includes identifying family members or friends who can provide practical help, arranging for postpartum childcare assistance, and connecting with other new mothers through prenatal classes or community groups.
Sleep management strategies acknowledge that while complete sleep deprivation is unavoidable with a newborn, optimizing rest opportunities can help maintain mental health. Strategies include accepting help with nighttime feedings, sleeping when the baby sleeps, and sharing overnight responsibilities with partners when possible.
Partner and family education about postpartum depression signs helps ensure that support people can recognize when professional help is needed. Partners play a crucial role in supporting new mothers and advocating for appropriate care when necessary.
Nutritional support includes maintaining adequate nutrition during the postpartum period, particularly for breastfeeding mothers. Some research suggests that omega-3 fatty acid supplementation and maintaining adequate vitamin D levels may help protect against postpartum depression.
Gradual return to physical activity and self-care routines supports both physical health and mental wellbeing. Even light exercise like walking can help improve mood and energy levels as recovery progresses.
FAQ
Is TMS safe while breastfeeding?
Yes, TMS is completely safe for breastfeeding mothers. Unlike antidepressant medications, TMS doesn’t introduce any substances into the bloodstream that could transfer to breast milk. The magnetic fields used in treatment are localized to specific brain areas and don’t affect other body systems or milk production. This makes TMS an ideal treatment option for mothers who want to continue breastfeeding while receiving effective depression treatment.
Can TMS be used if I’m already taking antidepressants?
Yes, TMS can be safely combined with antidepressant medications and may actually enhance treatment effectiveness. Some patients use TMS as an add-on therapy to boost the effects of medications that aren’t providing complete relief. Others may work with their healthcare providers to gradually taper antidepressant medications while receiving TMS treatment. The decision about combining or transitioning between treatments should always be made in consultation with qualified healthcare providers who can monitor progress and adjust treatment plans accordingly. Schedule a consultation today to talk with one of our experienced providers.
What happens if my postpartum depression returns after TMS treatment?
TMS treatment protocols often include maintenance sessions to prevent symptom recurrence. If depression symptoms return after successful TMS treatment, patients can typically receive additional TMS sessions or “booster” treatments. The maintenance schedule varies by individual but might involve weekly or monthly sessions for several months following the initial treatment course. Many patients find that maintenance TMS treatments are highly effective at preventing relapse and maintaining the improvements achieved during acute treatment.
Does insurance cover TMS for postpartum depression?
Standard TMS Therapy is covered by most insurance companies. If your insurance provider is not presently covering TMS, Acacia can help you negotiate with your insurance provider for reimbursement, on a case-by-case basis. Acacia has private pay options for all of our services, including TMS and Accelerated TMS. Acacia is pleased to provide financial aid for those who would benefit from TMS but may not be eligible for insurance coverage, or do not have insurance. Please contact us for more information.